
Suspected Microorganism
Salmonella
One of the most common pathogens found in people who are diagnosed with diarrhea is Salmonella. Below is a brief overview of this pathogen and some of its characteristics .
Characteristics
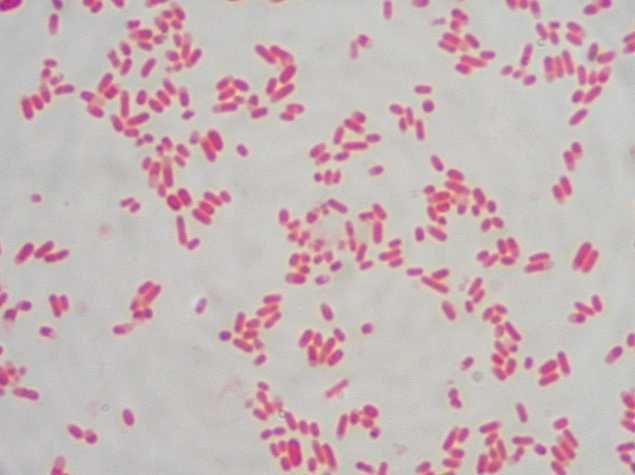
Salmonella is a Gram-negative facultative rod-shaped bacterium in the same proteobacterial family as Escherichia coli, the family Enterobacteriaceae, trivially known as "enteric" bacteria. Salmonella is nearly as well-studied as E. coli from a structural, biochemical and molecular point of view, and as poorly understood as E. coli from an ecological point of view. Salmonellae live in the intestinal tracts of warm and cold blooded animals. Some species are ubiquitous. Other species are specifically adapted to a particular host. In humans, Salmonella are the cause of two diseases called salmonellosis: enteric fever (typhoid), resulting from bacterial invasion of the bloodstream, and acute gastroenteritis, resulting from a foodborne infection/intoxication.
Salmonella Nomenclature
The genus Salmonella is a member of the family Enterobacteriaceae, It is composed of bacteria related to each other both phenotypically and genotypically. Salmonella DNA base composition is 50-52 mol% G+C, similar to that of Escherichia, Shigella, and Citrobacter. The bacteria of the genus Salmonella are also related to each other by DNA sequence. The genera with DNA most closely related to Salmonella are Escherichia, Shigella, and Citrobacter. Similar relationships were found by numerical taxonomy and 16S ssRNA analysis.
Salmonella nomenclature has been controversial since the original taxonomy of the genus was not based on DNA relatedness, rather names were given according to clinical considerations, e.g., Salmonella typhi, Salmonella cholerae-suis, Salmonella abortus-ovis, and so on. When serological analysis was adopted into the Kauffmann-White scheme in 1946, a Salmonella species was defined as "a group of related fermentation phage-type" with the result that each Salmonella serovar was considered as a species. Since the host-specificity suggested by some of these earlier names does not exist (e.g., S. typhi-murium, S. cholerae-suis are in fact ubiquitous), names derived from the geographical origin of the first isolated strain of the newly discovered serovars were next chosen, e.g., S. london, S. panama, S. stanleyville.
Susequently it was found that all Salmonella serovars form a single DNA hybridization group, i.e., a single species composed of seven subspecies, and thenomenclature had to be adapted. To avoid confusion with the familiar names of serovars, the species name Salmonella enterica was proposed with the following names for the subspecies:
enterica I
salamae II
arizonae IIIa
diarizonae IIIb
houtenae IV
bongori V
indica VI
Each subspecies contains various serovars defined by a characteristic antigenic formula.
Since this formal Latin nomenclature may not be clearly understood by physicians and epidemiologists, who are the most familiar with the names given to the most common serovars, the common serovars names are kept for subspecies I strains, which represent more than 99.5% of the Salmonella strains isolated from humans and other warm-blooded animals. The vernacular terminology seems preferred in medical practice, e.g., Salmonella ser. Typhimurium (not italicized) or shorter Salmonella (or S.) Typhimurium.
Habitats
The principal habitat of the salmonellae is the intestinal tract of humans and animals. Salmonella serovars can be found predominantly in one particular host, can be ubiquitous, or can have an unknown habitat. Typhi and Paratyphi A are strictly human serovars that may cause grave diseases often associated with invasion of the bloodstream. Salmonellosis in these cases is transmitted through fecal contamination of water or food. Gallinarum, Abortusovis, and Typhisuis are, respectively, avian, ovine, and porcine Salmonella serovars. Such host-adapted serovars cannot grow on minimal medium without growth factors (contrary to the ubiquitous Salmonella serovars).
Ubiquitous (non-host-adapted) Salmonella serovars (e.g., Typhimurium) cause very diverse clinical symptoms, from asymptomatic infection to serious typhoid-like syndromes in infants or certain highly susceptible animals (mice). In human adults, ubiquitousi organisms are mostly responsible for foodborne toxic infections.
The pathogenic role of a number of Salmonella serovars is unknown. This is especially the case with serovars from subspecies II to VI. A number of these serovars have been isolated rarely (some only once) during a systematic search in cold-blooded animals.
Salmonella in the Natural Environment
Salmonellae are disseminated in the natural environment (water, soil, sometimes plants used as food) through human or animal excretion. Humans and animals (either wild or domesticated) can excrete Salmonella either when clinically diseased or after having had salmonellosis, if they remain carriers. Salmonella organisms do not seem to multiply significantly in the natural environment (out of digestive tracts), but they can survive several weeks in water and several years in soil if conditions of temperature, humidity, and pH are favorable.
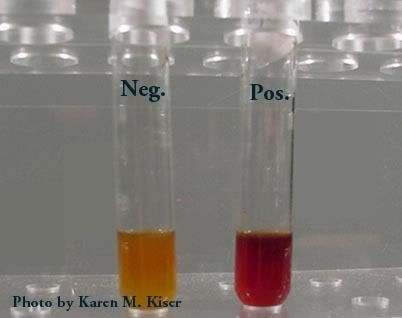
Isolation and Identification of Salmonella
A number of plating media have been devised for the isolation of Salmonella. Some media are differential and nonselective, i.e., they contain lactose with a pH indicator, but do not contain any inhibitor for non salmonellae (e.g., bromocresol purple lactose agar). Other media are differential and slightly selective, i.e., in addition to lactose and a pH indicator, they contain an inhibitor for nonenterics (e.g., MacConkey agar and eosin-methylene blue agar).
The most commonly used media selective for Salmonella are SS agar, bismuth sulfite agar, Hektoen enteric (HE) medium, brilliant green agar and xylose-lisine-deoxycholate (XLD) agar. All these media contain both selective and differential ingredients and they are commercially available.
Media used for Salmonella identification are those used for identification of all Enterobacteriaceae. Most Salmonella strains are motile with peritrichous flagella, however, nonmotile variants may occur occasionally. Most strains grow on nutrient agar as smooth colonies, 2-4 mm in diameter. Most strains are prototrophs, not requiring any growth factors. However, auxotrophic strains do occur, especially in host-adapted serovars such as Typhi and Paratyphi A.
Pathogenesis of Salmomella Infections in Humans
Salmonella infections in humans vary with the serovar, the strain, the infectious dose, the nature of the contaminated food, and the host status. Certain serovars are highly pathogenic for humans; the virulence of more rare serovars is unknown. Strains of the same serovar are also known to differ in their pathogenicity. An oral dose of at least 105Salmonella Typhi cells are needed to cause typhoid in 50% of human volunteers, whereas at least 109 S. Typhimurium cells (oral dose) are needed to cause symptoms of a toxic infection. Infants, immunosuppressed patients, and those affected with blood disease are more susceptible to Salmonella infection than healthy adults.
In the pathogenesis of typhoid the bacteria enter the human digestive tract, penetrate the intestinal mucosa (causing no lesion), and are stopped in the mesenteric lymph nodes. There, bacterial multiplication occurs, and part of the bacterial population lyses. From the mesenteric lymph nodes, viable bacteria and LPS (endotoxin) may be released into the bloodstream resulting in septicemia Release of endotoxin is responsible for cardiovascular “collapsus and tuphos” (a stuporous state—origin of the name typhoid) due to action on the ventriculus neurovegetative centers.
Salmonella excretion by human patients may continue long after clinical cure. Asymptomatic carriers are potentially dangerous when unnoticed. About 5% of patients clinically cured from typhoid remain carriers for months or even years. Antibiotics are usually ineffective on Salmonella carriage (even if salmonellae are susceptible to them) because the site of carriage may not allow penetration by the antibiotic.
Salmonellae survive sewage treatments if suitable germicides are not used in sewage processing. In a typical cycle of typhoid, sewage from a community is directed to a sewage plant. Effluent from the sewage plant passes into a coastal river where edible shellfish (mussels, oysters) live. Shellfish concentrate bacteria as they filter several liters of water per hour. Ingestion by humans of these seafoods (uncooked or superficially cooked) may cause typhoid or other salmonellosis. Salmonellae do not colonize or multiply in contaminated shellfish.
Typhoid is strictly a human disease.The incidence of human disease decreases when the level of development of a country increases (i.e., controlled water sewage systems, pasteurization of milk and dairy products). Where these hygienic conditions are missing, the probability of fecal contamination of water and food remains high and so is the incidence of typhoid.
Foodborne Salmonella toxic infections are caused by ubiquitous Salmonella serovars (e.g., Typhimurium). About 12-24 hours following ingestion of contaminated food (containing a sufficient number of Salmonella), symptoms appear (diarrhea, vomiting, fever) and last 2-5 days. Spontaneous cure usually occurs.
Salmonella may be associated with all kinds of food. Contamination of meat (cattle, pigs, goats, chicken, etc.) may originate from animal salmonellosis, but most often it results from contamination of muscles with the intestinal contents during evisceration of animals, washing, and transportation of carcasses. Surface contamination of meat is usually of little consequence, as proper cooking will sterilize it (although handling of contaminated meat may result in contamination of hands, tables, kitchenware, towels, other foods, etc.). However, when contaminated meat is ground, multiplication of Salmonella may occur within the ground meat and if cooking is superficial, ingestion of this highly contaminated food may produce a Salmonella infection. Infection may follow ingestion of any food that supports multiplication of Salmonella such as eggs, cream, mayonnaise, creamed foods, etc.), as a large number of ingested salmonellae are needed to give symptoms. Prevention of Salmonella toxic infection relies on avoiding contamination (improvement of hygiene), preventing multiplication of Salmonella in food (constant storage of food at 4°C), and use of pasteurized and sterilized milk and milk products. Vegetables and fruits may carry Salmonella when contaminated with fertilizers of fecal origin, or when washed with polluted water.
The incidence of foodborne Salmonella infection/toxication remains reletavely high in developed countries because of commercially prepared food or ingredients for food. Any contamination of commercially prepared food will result in a large-scale infection. In underdeveloped countries, foodborne Salmonella intoxications are less spectacular because of the smaller number of individuals simultaneously infected, but also because the bacteriological diagnosis of Salmonella toxic infection may not be available. However, the incidence of Salmonella carriage in underdeveloped countries is known to be high.
Salmonella epidemics may occur among infants in pediatric wards. The frequency and gravity of these epidemics are affected by hygienic conditions, malnutrition, and the excessive use of antibiotics that select for multiresistant strains.
Salmonella Enteritidis Infection
Egg-associated salmonellosis is an important public health problem in the United States and several European countries. Salmonella Enteritidis, can be inside perfectly normal-appearing eggs, and if the eggs are eaten raw or undercooked, the bacterium can cause illness. During the 1980s, illness related to contaminated eggs occurred mosy frequently in the northeastern United States, but now illness caused by S. Enteritidis is increasing in other parts of the country as well.
Unlike eggborne salmonellosis of past decades, the current epidemic is due to intact and disinfected grade A eggs. Salmonella Enteritidis silently infects the ovaries of healthy appearing hens and contaminates the eggs before the shells are formed. Most types of Salmonella live in the intestinal tracts of animals and birds and are transmitted to humans by contaminated foods of animal origin. Stringent procedures for cleaning and inspecting eggs were implemented in the 1970s and have made salmonellosis caused by external fecal contamination of egg shells extremely rare. However, unlike eggborne salmonellosis of past decades, the current epidemic is due to intact and disinfected grade A eggs. The reason for this is that Salmonella Enteritidis silently infects the ovaries of hens and contaminates the eggs before the shells are formed.
Although most infected hens have been found in the northeastern United States, the infection also occurs in hens in other areas of the country. In the Northeast, approximately one in 10,000 eggs may be internally contaminated. In other parts of the United States, contaminated eggs appear less common. Only a small number of hens seem to be infected at any given time, and an infected hen can lay many normal eggs while only occasionally laying an egg contaminated with Salmonella Enteritidis.
A person infected with the Salmonella Enteritidis usually has fever, abdominal cramps, and diarrhea beginning 12 to 72 hours after consuming a contaminated food or beverage. The illness usually lasts 4 to 7 days, and most persons recover without antibiotic treatment. However, the diarrhea can be severe, and the person may be ill enough to require hospitalization. The elderly, infants, and those with impaired immune systems (including HIV) may have a more severe illness. In these patients, the infection may spread from the intestines to the bloodstream, and then to other body sites and can cause death unless the person is treated promptly with antibiotics.
Exotoxins
Salmonella strains may produce a thermolabile enterotoxin that bears a limited relatedness to cholera toxin both structurally and antigenically. This enterotoxin causes water secretion in rat ileal loop and is recognized by antibodies against both cholera toxin and the thermolabile enterotoxin (LT) of enterotoxinogenic E. coli, but it does not bind in vitro to ganglioside GM1 (the receptor for E. coli LT and cholera ctx). Additionally, a cytotoxin that inhibits protein synthesis and is immunologically distinct from Shiga toxin has been demonstrated. Both of these toxins are presumed to play a role in the diarrheal symptoms of salmonellosis.
Antibiotic Susceptibility
During the last decade, antibiotic resistance and multiresistance of Salmonella spp. have increased a great deal. The cause appears to be the increased and indiscriminate use of antibiotics in the treatment of humans and animals and the addition of growth-promoting antibiotics to the food of breeding animals. Plasmid-borne antibiotic resistance is very frequent among Salmonella strains involved in pediatric epidemics (e.g., Typhimurium, Panama, Wien, Infantis). Resistance to ampicillin, streptomycin, kanamycin, chloramphenicol, tetracycline, and sulfonamides is commonly observed. Colistin resistance has not yet been observed.
Additional Info
Background: First described in 1880 and cultured in 1884, salmonellae are motile, gram-negative, rod-shaped bacteria of the family Enterobacteriaceae. Named after Daniel E. Salmon, the pathologist who first isolated the organism from porcine intestine, salmonellae are common in the gastrointestinal tracts of mammals, reptiles, birds, and insects.
As with the closely related bacterium Escherichia coli, salmonellae are potential enteric pathogens and a leading cause of bacterial food-borne illness. Additionally, salmonellae have been implicated in a spectrum of other diseases, including enteric or typhoid fever (primarily Salmonella typhi and Salmonella paratyphi), bacteremia, endovascular infections, focal infections (eg, osteomyelitis), and enterocolitis (typically Salmonella typhimurium, Salmonella enteritidis, and Salmonella heidelberg).
All salmonellae are grouped into a single overarching species. This species, Salmonella choleraesuis, is divided into 7 subgroups based on DNA homology and host range. Most of the salmonellae that are pathogenic in humans belong to a single subgroup (subgroup I). Additionally, each of the salmonellae can be serotyped according to their particular complement of somatic O, surface Vi, and flagellar H antigens. Presently, more than 2,300 Salmonella serovars exist.
Salmonellae can be isolated in the microbiology laboratory using a number of low-selective media (MacConkey agar, deoxycholate agar), intermediate-selective media (Salmonella-Shigella [SS] agar, Hektoen [HE] agar), and highly selective media (selenite agar with brilliant green). Individual isolates can then be distinguished by serotyping, bacteriophage typing, and genotyping.
Pathophysiology: The transmission of salmonellae to a susceptible host usually occurs by consumption of contaminated foods. The most common sources of salmonellae are beef, poultry, and eggs. In one recent estimate, consumption of egg shell fragments contaminated with Salmonella enterica serovar Enteritidis was responsible for approximately 182,060 cases of enteritis in the United States in the year 2000. Improperly prepared fruits, vegetables, dairy products, and shellfish have also been implicated as sources of Salmonella. Moreover, human-to-human and animal-to-human transmission can occur. For example, amphibian and reptile exposure is associated with approximately 74,000 Salmonella infections annually in the United States. Recently, cats have also been implicated as a potential reservoir.
Although the infectious dose varies among strains, a large inoculum is thought to be necessary to overcome stomach acidity and to compete with normal intestinal flora. Large inocula are also associated with higher rates of illness and shorter incubation periods. However, lower infectious doses may be adequate to cause infection if these organisms are co-ingested with foods that rapidly transit the stomach (eg, liquids) or that raise gastric pH (eg, cheese, milk), if antacids are used concomitantly, or if these organisms are ingested by individuals with impaired immune systems.
After ingestion, infection with salmonellae is characterized by attachment of the bacteria by fimbriae or pili to cells lining the intestinal lumen. Salmonellae selectively attach to specialized epithelial cells (M cells) of the Peyer patches. The bacteria are then internalized by receptor-mediated endocytosis and transported within phagosomes to the lamina propria, where they are released. Once there, salmonellae induce an influx of macrophages (typhoidal strains) or neutrophils (nontyphoidal strains). Although nontyphoid salmonellae generally precipitate a localized response, S typhi and other especially virulent strains invade deeper tissues via lymphatics and capillaries and elicit a major immune response.
Virulence factors of salmonellae are complex and encoded both on the organism's chromosome and on large (34-120 kd) plasmids. Some areas of active investigation include the means by which salmonellae attach to and invade the intestine, survive within phagosomes, effect a massive efflux of electrolytes and water into the intestinal lumen, and develop drug resistance. Several Salmonella pathogenicity islands have been identified that mediate uptake of the bacteria into epithelial cells (type III secretion system [TTSS]), nonphagocytic cell invasion (Salmonella pathogenicity-island 1 [SPI-1]), and survival and replication within macrophages (Salmonella pathogenicity-island 2 [SPI-2], phoP/phoQ).
The severity of illness in individuals infected with salmonellae is determined not only by the virulence factors of the infecting strain but by host properties as well. For example, individuals at the extremes of age (ie, people who are very young or very old) are at an increased risk for bacteremia. Similarly, systemic lupus erythematosus, malignancies, and immune deficiency are also associated with increased risk of bacteremia.
History: salmonella infections typically produce 1 of 3 distinct syndromes: gastroenteritis, typhoid (enteric) fever, or focal disease.
Infection with nontyphoidal salmonellae usually causes enterocolitis similar to that caused by other bacterial enteric pathogens.
Nausea, vomiting, and diarrhea occur within 6-48 hours after ingestion of contaminated food or drink.
In most cases, stools are loose and bloodless. Salmonellae may rarely cause large-volume choleralike diarrhea or may be associated with tenesmus.
The diarrhea is typically self-limiting and resolves within 3-7 days.
While an initial transient diarrhea may occur, established infections with S typhi or S paratyphi are associated with abdominal pain and either constipation (~40%) or recurrent diarrhea (~40%).
Fever, abdominal cramping, chills, headache, and myalgia are common.
Fever usually resolves within 48 hours.
Enteric fever (typically caused by S typhi or S paratyphi) is generally an acute illness manifested by fever, headache, and abdominal symptoms and should be considered in travelers returning from tropical and subtropical areas.
Focal disease is variable and defined by the site of infection.
Physical: Patients with Salmonella gastroenteritis typically have a self-limiting fever (38-39°C) within 48 hours of ingestion. A prolonged persistent fever (4-8 wk in untreated individuals) that increases daily (as high as 41°C) suggests typhoid fever. Nontyphoidal gastroenteritis is generally limited to diarrhea, although typhoid (enteric) fever may present with both gastrointestinal and skin manifestations (ie, rose spots). The following organ systems may be involved with Salmonella infection:
Gastrointestinal: Salmonella infections typically cause nonbloody loose stool or watery diarrhea. Abdominal tenderness (~50%) and mild hepatosplenomegaly (~50%) are both common in patients with typhoid fever.
Cardiovascular: Salmonella infections (commonly S typhimurium or S choleraesuis) may produce arterial infections or endocarditis.
Pulmonary: Salmonella pneumonia or empyema is rare in the absence of comorbid illnesses such as underlying lung disease, malignancy, diabetes, sickle cell anemia, or alcohol abuse.
Genitourinary: Individuals with urolithiasis or structural abnormalities or individuals who are undergoing immunosuppressive therapy are predisposed to Salmonella urinary tract infections.
Neurologic: Salmonella meningitis may rarely occur, typically in infants and young children.
Skeletal: Infection with salmonellae may cause septic arthritis and osteomyelitis. The latter affects the long bones and typically occurs in patients with sickle cell disease.
Integument: Enteric fever may be associated with pink, blanchable, slightly raised macules (rose spots) on the chest and abdomen.
The causative agent of typhoid fever is the bacterium Salmonella typhi. (Image courtesy of the Centers for Disease Control and Prevention
References:
>medlineplus>>ency>>imagepages>>1048.htm">http>>www.nlm.nih.gov>>medlineplus>>ency>>imagepages>>1048.htm
>MED>>topic2058.htm">http>>www.emedicine.com>>MED>>topic2058.htm
Salmonella
One of the most common pathogens found in people who are diagnosed with diarrhea is Salmonella. Below is a brief overview of this pathogen and some of its characteristics .
Characteristics
Salmonella is a Gram-negative facultative rod-shaped bacterium in the same proteobacterial family as Escherichia coli, the family Enterobacteriaceae, trivially known as "enteric" bacteria. Salmonella is nearly as well-studied as E. coli from a structural, biochemical and molecular point of view, and as poorly understood as E. coli from an ecological point of view. Salmonellae live in the intestinal tracts of warm and cold blooded animals. Some species are ubiquitous. Other species are specifically adapted to a particular host. In humans, Salmonella are the cause of two diseases called salmonellosis: enteric fever (typhoid), resulting from bacterial invasion of the bloodstream, and acute gastroenteritis, resulting from a foodborne infection/intoxication.
Salmonella Nomenclature
The genus Salmonella is a member of the family Enterobacteriaceae, It is composed of bacteria related to each other both phenotypically and genotypically. Salmonella DNA base composition is 50-52 mol% G+C, similar to that of Escherichia, Shigella, and Citrobacter. The bacteria of the genus Salmonella are also related to each other by DNA sequence. The genera with DNA most closely related to Salmonella are Escherichia, Shigella, and Citrobacter. Similar relationships were found by numerical taxonomy and 16S ssRNA analysis.
Salmonella nomenclature has been controversial since the original taxonomy of the genus was not based on DNA relatedness, rather names were given according to clinical considerations, e.g., Salmonella typhi, Salmonella cholerae-suis, Salmonella abortus-ovis, and so on. When serological analysis was adopted into the Kauffmann-White scheme in 1946, a Salmonella species was defined as "a group of related fermentation phage-type" with the result that each Salmonella serovar was considered as a species. Since the host-specificity suggested by some of these earlier names does not exist (e.g., S. typhi-murium, S. cholerae-suis are in fact ubiquitous), names derived from the geographical origin of the first isolated strain of the newly discovered serovars were next chosen, e.g., S. london, S. panama, S. stanleyville.
Susequently it was found that all Salmonella serovars form a single DNA hybridization group, i.e., a single species composed of seven subspecies, and thenomenclature had to be adapted. To avoid confusion with the familiar names of serovars, the species name Salmonella enterica was proposed with the following names for the subspecies:
enterica I
salamae II
arizonae IIIa
diarizonae IIIb
houtenae IV
bongori V
indica VI
Each subspecies contains various serovars defined by a characteristic antigenic formula.
Since this formal Latin nomenclature may not be clearly understood by physicians and epidemiologists, who are the most familiar with the names given to the most common serovars, the common serovars names are kept for subspecies I strains, which represent more than 99.5% of the Salmonella strains isolated from humans and other warm-blooded animals. The vernacular terminology seems preferred in medical practice, e.g., Salmonella ser. Typhimurium (not italicized) or shorter Salmonella (or S.) Typhimurium.
Habitats
The principal habitat of the salmonellae is the intestinal tract of humans and animals. Salmonella serovars can be found predominantly in one particular host, can be ubiquitous, or can have an unknown habitat. Typhi and Paratyphi A are strictly human serovars that may cause grave diseases often associated with invasion of the bloodstream. Salmonellosis in these cases is transmitted through fecal contamination of water or food. Gallinarum, Abortusovis, and Typhisuis are, respectively, avian, ovine, and porcine Salmonella serovars. Such host-adapted serovars cannot grow on minimal medium without growth factors (contrary to the ubiquitous Salmonella serovars).
Ubiquitous (non-host-adapted) Salmonella serovars (e.g., Typhimurium) cause very diverse clinical symptoms, from asymptomatic infection to serious typhoid-like syndromes in infants or certain highly susceptible animals (mice). In human adults, ubiquitousi organisms are mostly responsible for foodborne toxic infections.
The pathogenic role of a number of Salmonella serovars is unknown. This is especially the case with serovars from subspecies II to VI. A number of these serovars have been isolated rarely (some only once) during a systematic search in cold-blooded animals.
Salmonella in the Natural Environment
Salmonellae are disseminated in the natural environment (water, soil, sometimes plants used as food) through human or animal excretion. Humans and animals (either wild or domesticated) can excrete Salmonella either when clinically diseased or after having had salmonellosis, if they remain carriers. Salmonella organisms do not seem to multiply significantly in the natural environment (out of digestive tracts), but they can survive several weeks in water and several years in soil if conditions of temperature, humidity, and pH are favorable.
Isolation and Identification of Salmonella
A number of plating media have been devised for the isolation of Salmonella. Some media are differential and nonselective, i.e., they contain lactose with a pH indicator, but do not contain any inhibitor for non salmonellae (e.g., bromocresol purple lactose agar). Other media are differential and slightly selective, i.e., in addition to lactose and a pH indicator, they contain an inhibitor for nonenterics (e.g., MacConkey agar and eosin-methylene blue agar).
The most commonly used media selective for Salmonella are SS agar, bismuth sulfite agar, Hektoen enteric (HE) medium, brilliant green agar and xylose-lisine-deoxycholate (XLD) agar. All these media contain both selective and differential ingredients and they are commercially available.
Media used for Salmonella identification are those used for identification of all Enterobacteriaceae. Most Salmonella strains are motile with peritrichous flagella, however, nonmotile variants may occur occasionally. Most strains grow on nutrient agar as smooth colonies, 2-4 mm in diameter. Most strains are prototrophs, not requiring any growth factors. However, auxotrophic strains do occur, especially in host-adapted serovars such as Typhi and Paratyphi A.
Pathogenesis of Salmomella Infections in Humans
Salmonella infections in humans vary with the serovar, the strain, the infectious dose, the nature of the contaminated food, and the host status. Certain serovars are highly pathogenic for humans; the virulence of more rare serovars is unknown. Strains of the same serovar are also known to differ in their pathogenicity. An oral dose of at least 105Salmonella Typhi cells are needed to cause typhoid in 50% of human volunteers, whereas at least 109 S. Typhimurium cells (oral dose) are needed to cause symptoms of a toxic infection. Infants, immunosuppressed patients, and those affected with blood disease are more susceptible to Salmonella infection than healthy adults.
In the pathogenesis of typhoid the bacteria enter the human digestive tract, penetrate the intestinal mucosa (causing no lesion), and are stopped in the mesenteric lymph nodes. There, bacterial multiplication occurs, and part of the bacterial population lyses. From the mesenteric lymph nodes, viable bacteria and LPS (endotoxin) may be released into the bloodstream resulting in septicemia Release of endotoxin is responsible for cardiovascular “collapsus and tuphos” (a stuporous state—origin of the name typhoid) due to action on the ventriculus neurovegetative centers.
Salmonella excretion by human patients may continue long after clinical cure. Asymptomatic carriers are potentially dangerous when unnoticed. About 5% of patients clinically cured from typhoid remain carriers for months or even years. Antibiotics are usually ineffective on Salmonella carriage (even if salmonellae are susceptible to them) because the site of carriage may not allow penetration by the antibiotic.
Salmonellae survive sewage treatments if suitable germicides are not used in sewage processing. In a typical cycle of typhoid, sewage from a community is directed to a sewage plant. Effluent from the sewage plant passes into a coastal river where edible shellfish (mussels, oysters) live. Shellfish concentrate bacteria as they filter several liters of water per hour. Ingestion by humans of these seafoods (uncooked or superficially cooked) may cause typhoid or other salmonellosis. Salmonellae do not colonize or multiply in contaminated shellfish.
Typhoid is strictly a human disease.The incidence of human disease decreases when the level of development of a country increases (i.e., controlled water sewage systems, pasteurization of milk and dairy products). Where these hygienic conditions are missing, the probability of fecal contamination of water and food remains high and so is the incidence of typhoid.
Foodborne Salmonella toxic infections are caused by ubiquitous Salmonella serovars (e.g., Typhimurium). About 12-24 hours following ingestion of contaminated food (containing a sufficient number of Salmonella), symptoms appear (diarrhea, vomiting, fever) and last 2-5 days. Spontaneous cure usually occurs.
Salmonella may be associated with all kinds of food. Contamination of meat (cattle, pigs, goats, chicken, etc.) may originate from animal salmonellosis, but most often it results from contamination of muscles with the intestinal contents during evisceration of animals, washing, and transportation of carcasses. Surface contamination of meat is usually of little consequence, as proper cooking will sterilize it (although handling of contaminated meat may result in contamination of hands, tables, kitchenware, towels, other foods, etc.). However, when contaminated meat is ground, multiplication of Salmonella may occur within the ground meat and if cooking is superficial, ingestion of this highly contaminated food may produce a Salmonella infection. Infection may follow ingestion of any food that supports multiplication of Salmonella such as eggs, cream, mayonnaise, creamed foods, etc.), as a large number of ingested salmonellae are needed to give symptoms. Prevention of Salmonella toxic infection relies on avoiding contamination (improvement of hygiene), preventing multiplication of Salmonella in food (constant storage of food at 4°C), and use of pasteurized and sterilized milk and milk products. Vegetables and fruits may carry Salmonella when contaminated with fertilizers of fecal origin, or when washed with polluted water.
The incidence of foodborne Salmonella infection/toxication remains reletavely high in developed countries because of commercially prepared food or ingredients for food. Any contamination of commercially prepared food will result in a large-scale infection. In underdeveloped countries, foodborne Salmonella intoxications are less spectacular because of the smaller number of individuals simultaneously infected, but also because the bacteriological diagnosis of Salmonella toxic infection may not be available. However, the incidence of Salmonella carriage in underdeveloped countries is known to be high.
Salmonella epidemics may occur among infants in pediatric wards. The frequency and gravity of these epidemics are affected by hygienic conditions, malnutrition, and the excessive use of antibiotics that select for multiresistant strains.
Salmonella Enteritidis Infection
Egg-associated salmonellosis is an important public health problem in the United States and several European countries. Salmonella Enteritidis, can be inside perfectly normal-appearing eggs, and if the eggs are eaten raw or undercooked, the bacterium can cause illness. During the 1980s, illness related to contaminated eggs occurred mosy frequently in the northeastern United States, but now illness caused by S. Enteritidis is increasing in other parts of the country as well.
Unlike eggborne salmonellosis of past decades, the current epidemic is due to intact and disinfected grade A eggs. Salmonella Enteritidis silently infects the ovaries of healthy appearing hens and contaminates the eggs before the shells are formed. Most types of Salmonella live in the intestinal tracts of animals and birds and are transmitted to humans by contaminated foods of animal origin. Stringent procedures for cleaning and inspecting eggs were implemented in the 1970s and have made salmonellosis caused by external fecal contamination of egg shells extremely rare. However, unlike eggborne salmonellosis of past decades, the current epidemic is due to intact and disinfected grade A eggs. The reason for this is that Salmonella Enteritidis silently infects the ovaries of hens and contaminates the eggs before the shells are formed.
Although most infected hens have been found in the northeastern United States, the infection also occurs in hens in other areas of the country. In the Northeast, approximately one in 10,000 eggs may be internally contaminated. In other parts of the United States, contaminated eggs appear less common. Only a small number of hens seem to be infected at any given time, and an infected hen can lay many normal eggs while only occasionally laying an egg contaminated with Salmonella Enteritidis.
A person infected with the Salmonella Enteritidis usually has fever, abdominal cramps, and diarrhea beginning 12 to 72 hours after consuming a contaminated food or beverage. The illness usually lasts 4 to 7 days, and most persons recover without antibiotic treatment. However, the diarrhea can be severe, and the person may be ill enough to require hospitalization. The elderly, infants, and those with impaired immune systems (including HIV) may have a more severe illness. In these patients, the infection may spread from the intestines to the bloodstream, and then to other body sites and can cause death unless the person is treated promptly with antibiotics.
Exotoxins
Salmonella strains may produce a thermolabile enterotoxin that bears a limited relatedness to cholera toxin both structurally and antigenically. This enterotoxin causes water secretion in rat ileal loop and is recognized by antibodies against both cholera toxin and the thermolabile enterotoxin (LT) of enterotoxinogenic E. coli, but it does not bind in vitro to ganglioside GM1 (the receptor for E. coli LT and cholera ctx). Additionally, a cytotoxin that inhibits protein synthesis and is immunologically distinct from Shiga toxin has been demonstrated. Both of these toxins are presumed to play a role in the diarrheal symptoms of salmonellosis.
Antibiotic Susceptibility
During the last decade, antibiotic resistance and multiresistance of Salmonella spp. have increased a great deal. The cause appears to be the increased and indiscriminate use of antibiotics in the treatment of humans and animals and the addition of growth-promoting antibiotics to the food of breeding animals. Plasmid-borne antibiotic resistance is very frequent among Salmonella strains involved in pediatric epidemics (e.g., Typhimurium, Panama, Wien, Infantis). Resistance to ampicillin, streptomycin, kanamycin, chloramphenicol, tetracycline, and sulfonamides is commonly observed. Colistin resistance has not yet been observed.
Additional Info
Background: First described in 1880 and cultured in 1884, salmonellae are motile, gram-negative, rod-shaped bacteria of the family Enterobacteriaceae. Named after Daniel E. Salmon, the pathologist who first isolated the organism from porcine intestine, salmonellae are common in the gastrointestinal tracts of mammals, reptiles, birds, and insects.
As with the closely related bacterium Escherichia coli, salmonellae are potential enteric pathogens and a leading cause of bacterial food-borne illness. Additionally, salmonellae have been implicated in a spectrum of other diseases, including enteric or typhoid fever (primarily Salmonella typhi and Salmonella paratyphi), bacteremia, endovascular infections, focal infections (eg, osteomyelitis), and enterocolitis (typically Salmonella typhimurium, Salmonella enteritidis, and Salmonella heidelberg).
All salmonellae are grouped into a single overarching species. This species, Salmonella choleraesuis, is divided into 7 subgroups based on DNA homology and host range. Most of the salmonellae that are pathogenic in humans belong to a single subgroup (subgroup I). Additionally, each of the salmonellae can be serotyped according to their particular complement of somatic O, surface Vi, and flagellar H antigens. Presently, more than 2,300 Salmonella serovars exist.
Salmonellae can be isolated in the microbiology laboratory using a number of low-selective media (MacConkey agar, deoxycholate agar), intermediate-selective media (Salmonella-Shigella [SS] agar, Hektoen [HE] agar), and highly selective media (selenite agar with brilliant green). Individual isolates can then be distinguished by serotyping, bacteriophage typing, and genotyping.
Pathophysiology: The transmission of salmonellae to a susceptible host usually occurs by consumption of contaminated foods. The most common sources of salmonellae are beef, poultry, and eggs. In one recent estimate, consumption of egg shell fragments contaminated with Salmonella enterica serovar Enteritidis was responsible for approximately 182,060 cases of enteritis in the United States in the year 2000. Improperly prepared fruits, vegetables, dairy products, and shellfish have also been implicated as sources of Salmonella. Moreover, human-to-human and animal-to-human transmission can occur. For example, amphibian and reptile exposure is associated with approximately 74,000 Salmonella infections annually in the United States. Recently, cats have also been implicated as a potential reservoir.
Although the infectious dose varies among strains, a large inoculum is thought to be necessary to overcome stomach acidity and to compete with normal intestinal flora. Large inocula are also associated with higher rates of illness and shorter incubation periods. However, lower infectious doses may be adequate to cause infection if these organisms are co-ingested with foods that rapidly transit the stomach (eg, liquids) or that raise gastric pH (eg, cheese, milk), if antacids are used concomitantly, or if these organisms are ingested by individuals with impaired immune systems.
After ingestion, infection with salmonellae is characterized by attachment of the bacteria by fimbriae or pili to cells lining the intestinal lumen. Salmonellae selectively attach to specialized epithelial cells (M cells) of the Peyer patches. The bacteria are then internalized by receptor-mediated endocytosis and transported within phagosomes to the lamina propria, where they are released. Once there, salmonellae induce an influx of macrophages (typhoidal strains) or neutrophils (nontyphoidal strains). Although nontyphoid salmonellae generally precipitate a localized response, S typhi and other especially virulent strains invade deeper tissues via lymphatics and capillaries and elicit a major immune response.
Virulence factors of salmonellae are complex and encoded both on the organism's chromosome and on large (34-120 kd) plasmids. Some areas of active investigation include the means by which salmonellae attach to and invade the intestine, survive within phagosomes, effect a massive efflux of electrolytes and water into the intestinal lumen, and develop drug resistance. Several Salmonella pathogenicity islands have been identified that mediate uptake of the bacteria into epithelial cells (type III secretion system [TTSS]), nonphagocytic cell invasion (Salmonella pathogenicity-island 1 [SPI-1]), and survival and replication within macrophages (Salmonella pathogenicity-island 2 [SPI-2], phoP/phoQ).
The severity of illness in individuals infected with salmonellae is determined not only by the virulence factors of the infecting strain but by host properties as well. For example, individuals at the extremes of age (ie, people who are very young or very old) are at an increased risk for bacteremia. Similarly, systemic lupus erythematosus, malignancies, and immune deficiency are also associated with increased risk of bacteremia.
History: salmonella infections typically produce 1 of 3 distinct syndromes: gastroenteritis, typhoid (enteric) fever, or focal disease.
Infection with nontyphoidal salmonellae usually causes enterocolitis similar to that caused by other bacterial enteric pathogens.
Nausea, vomiting, and diarrhea occur within 6-48 hours after ingestion of contaminated food or drink.
In most cases, stools are loose and bloodless. Salmonellae may rarely cause large-volume choleralike diarrhea or may be associated with tenesmus.
The diarrhea is typically self-limiting and resolves within 3-7 days.
While an initial transient diarrhea may occur, established infections with S typhi or S paratyphi are associated with abdominal pain and either constipation (~40%) or recurrent diarrhea (~40%).
Fever, abdominal cramping, chills, headache, and myalgia are common.
Fever usually resolves within 48 hours.
Enteric fever (typically caused by S typhi or S paratyphi) is generally an acute illness manifested by fever, headache, and abdominal symptoms and should be considered in travelers returning from tropical and subtropical areas.
Focal disease is variable and defined by the site of infection.
Physical: Patients with Salmonella gastroenteritis typically have a self-limiting fever (38-39°C) within 48 hours of ingestion. A prolonged persistent fever (4-8 wk in untreated individuals) that increases daily (as high as 41°C) suggests typhoid fever. Nontyphoidal gastroenteritis is generally limited to diarrhea, although typhoid (enteric) fever may present with both gastrointestinal and skin manifestations (ie, rose spots). The following organ systems may be involved with Salmonella infection:
Gastrointestinal: Salmonella infections typically cause nonbloody loose stool or watery diarrhea. Abdominal tenderness (~50%) and mild hepatosplenomegaly (~50%) are both common in patients with typhoid fever.
Cardiovascular: Salmonella infections (commonly S typhimurium or S choleraesuis) may produce arterial infections or endocarditis.
Pulmonary: Salmonella pneumonia or empyema is rare in the absence of comorbid illnesses such as underlying lung disease, malignancy, diabetes, sickle cell anemia, or alcohol abuse.
Genitourinary: Individuals with urolithiasis or structural abnormalities or individuals who are undergoing immunosuppressive therapy are predisposed to Salmonella urinary tract infections.
Neurologic: Salmonella meningitis may rarely occur, typically in infants and young children.
Skeletal: Infection with salmonellae may cause septic arthritis and osteomyelitis. The latter affects the long bones and typically occurs in patients with sickle cell disease.
Integument: Enteric fever may be associated with pink, blanchable, slightly raised macules (rose spots) on the chest and abdomen.
The causative agent of typhoid fever is the bacterium Salmonella typhi. (Image courtesy of the Centers for Disease Control and Prevention
References:
>medlineplus>>ency>>imagepages>>1048.htm">http>>www.nlm.nih.gov>>medlineplus>>ency>>imagepages>>1048.htm
>MED>>topic2058.htm">http>>www.emedicine.com>>MED>>topic2058.htm










{kind=link}
{kind=link}
{kind=link}