
The table above is a summary of the 3 organisms chosen for the poster presentation.


Introduction: Fungal Infections
Fungi and yeasts are multi-celled plants that are parasites. An everyday example of a fungus is mushrooms. However, the fungi that cause human disease are usually very small fungi. There are a few common human fungal conditions that are rarely harmful except for those with severely weakened immune systems. (Source: WD Writers)
A fungus is actually a primitive vegetable. Fungi can be found in air, in soil, on plants, and in water. Thousands, perhaps millions, of different types of fungi exist on Earth. The most familiar ones to us are mushrooms, yeast, mold, and mildew. Some live in the human body, usually without causing illness. In fact, only about half of all types of fungi cause disease in humans. Those conditions are called mycoses. (Source: excerpt from Microbes in Sickness and in Health - Publications, National Institute of Allergy and Infectious Diseases: NIAID)
Definitions of Fungal Infections:
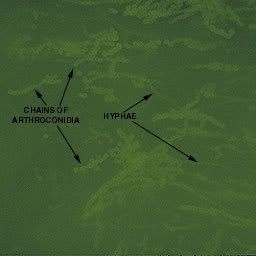
A kingdom of eukaryotic, heterotrophic organisms that live as saprobes or parasites, including mushrooms, yeasts, smuts, molds, etc. They reproduce either sexually or asexually, and have life cycles that range from simple to complex. Filamentous fungi refer to those that grow as multicellular colonies (mushrooms and molds).
Symptoms of fungal infections
Some of the symptoms of Fungal infections incude:
-Alopecia : various types of hair loss or balding
-Annular lesions
-Pustules : Small elevated pus containing lesion of the skin.
-Rash
-Onycholysis : Loosening or loss of part or all of nail.
Name and Aliases of Fungal Infections:
Main name of condition: Fungal infections
Other names or spellings for Fungal infections:
Fungi, Fungus, Fungal disease, Fungal diseases, Fungal condition, Fungal conditions, Mycoses, Mycosis, fungi, fungus Source - WD Writers
Types of Fungal Infections:
Subtypes of Fungal infections: Candida, Vaginal Candidiasis, Oral thrush, Athlete's foot, Tinea, Yeast infections, Ringworm, Allergic bronchopulmonary aspergillosis, Aspergillosis, Cryptococcal, Meningitis, Fungal nail infections, Histoplasmosis, invasive candidiasis, Mycetoma, Cryptococcosis, Sporotrichosis, Pityriasis Versicolor, Zygomycosis
Disease Category: Parasite.fungal
Parasite.fungal: Diseases caused by fungi Introduction: Fungi and yeasts are multi-celled plants that are parasites. An everyday example of a fungus is mushrooms. However, the fungi that cause human disease are usually very small fungi. There are a few common human fungal conditions that are rarely harmful except for those with severely weakened immune systems. Some examples are Candida (thrush), Yeast infections, Tinea (Athlete's foot), and Ringworm.
Risk Factors for Fungal infections
Risk factors for Fungal infections are factors that do not seem to be a direct cause of the disease, but seem to be associated in some way. Having a risk factor for Fungal infections makes the chances of getting a condition higher but does not always lead to Fungal infections. The list of risk factors mentioned for Fungal infections in various sources includes: Damaged skin, Moist skin, Broad-spectrum antibiotics, Immunocompromise, AIDS and Chronic disease.
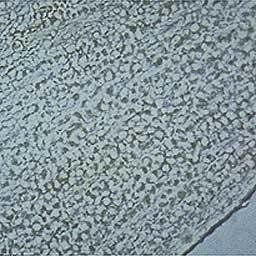




Pseudomonas aeruginosa on MacConkey agar
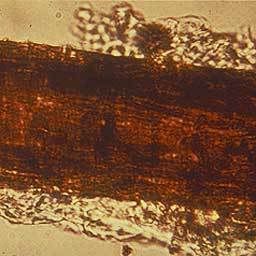
E.coli
E. coli is the head of the large bacterial family, Enterobacteriaceae, the enteric bacteria, which are faculatively anaerobic Gram-negative rods that live in the intestinal tracts of animals in health and disease. The Enterobacteriaceae are among the most important bacteria medically. A number of genera within the family are human intestinal pathogens (e.g. Salmonella, Shigella, Yersinia). Several others are normal colonists of the human gastrointestinal tract (e.g. Escherichia, Enterobacter, Klebsiella), but these bacteria, as well, may occasionally be associated with diseases of humans.
The Enterobacteriaceae are distinguished from the Pseudomonadaceae in a number of ways known reflexively to competent microbiologists. The pseudomonads are respiratory, never fermentative, oxidase-positive, and motile by means of polar flagella. The enterics ferment glucose producing acid and gas, are typically oxidase-negative, and when motile, produce peritrichous flagella.
Physiologically, E. coli is versatile and well-adapted to its characteristic habitats. It can grow in media with glucose as the sole organic constituent. Wild-type E. coli has no growth factor requirements, and metabolically it can transform glucose into all of the macromolecular components that make up the cell. The bacterium can grow in the presence or absence of O2. Under anaerobic conditions it will grow by means of fermentation, producing characteristic "mixed acids and gas" as end products. However, it can also grow by means of anaerobic respiration, since it is able to utilize NO3, NO2 or fumarate as final electron acceptors for respiratory electron transport processes. In part, this adapts E. coli to its intestinal (anaerobic) and its extraintestinal (aerobic or anaerobic) habitats.
E. coli can respond to environmental signals such as chemicals, pH, temperature, osmolarity, etc., in a number of very remarkable ways considering it is a single-celled organism. For example, it can sense the presence or absence of chemicals and gases in its environment and swim towards or away from them. Or it can stop swimming and grow fimbriae that will specifically attach it to a cell or surface receptor. In response to change in temperature and osmolarity, it can vary the pore diameter of its outer membrane porins to accommodate larger molecules (nutrients) or to exclude inhibitory substances. With its complex mechanisms for regulation of metabolism the bacterium can survey the chemical contents its environment in advance of synthesizing any enzymes necessary to use these compounds. It does not wastefully produce enzymes for degradation of carbon sources unless they are available, and it does not produce enzymes for synthesis of metabolites if they are available as nutrients in the environment.



{kind=link}